Designing where people already are
Field research, HCD facilitation and tool design for the WorkerHealth program, Phnom Penh and Kandal, 2017 to 2018.

In late 2017 I was in a garment factory infirmary on the edge of Phnom Penh. A low room with fluorescent lights and damp stains on the wooden wall panels. Eight beds, no mattresses, colored plastic mats on top. Health posters on the walls. The nurse was in her late forties, friendly, a white medical shirt pulled over her street clothes, her factory ID hanging from a Starbucks lanyard.
We asked how she knows when a worker needs sexual and reproductive health information. She told us the WorkerHealth Champions had a group chat on Facebook. They used it to flag workers who might need help and to stay connected with the clinic staff.
Nobody in the program had designed that. The workers built it themselves.
The program
A quarter of all Cambodian women between 18 and 29 work in garment factories, and at the time 80% of them were not using a modern method of family planning. WorkerHealth was Marie Stopes International Cambodia's response, funded by USAID and running in more than 30 factories: strengthened factory infirmaries, a referral network of quality-assured clinics, and trained volunteers called WorkerHealth Champions on the factory floor, a familiar face workers could ask about family planning.
The program was winding down. Marie Stopes brought Glean in to design tools that would let the whole system keep working after the project funding ended, for three groups: the infirmary and clinic staff, the Champions, and factory management.
Research on the factory floor
Blunt questions get cautious answers, especially about sexual health, and especially at work. So we built the research around roleplay and observation. A member of our team played a worker with morning sickness or a contraception question, and the infirmary or clinic staff responded the way they normally would. We watched what they actually did, then asked follow-up questions about what we'd seen. In group sessions we used experience mapping: participants ranked their experiences on a paper scale with post-it notes, silently, before any discussion, so the most senior voice in the room didn't set everyone else's answers.
On a single day we ran sessions in eight locations: four factory infirmaries and four clinics. A few weeks later we spent three mornings with Champions in three factories across Phnom Penh and Kandal, and the afternoons in the same factories with HR staff and management.
Not all of it went to plan. In our first factory session the participants weren't from HR at all, and a program staff member stayed in the room after we'd asked for the session to run without observers, so the junior participants gave careful non-answers. We rewrote the protocol before the next factory. Field research rarely follows the schedule you wrote in the office.
What we found
Trust was the biggest problem. Many workers didn't believe a conversation with a Champion would stay confidential. The Champions had no way of showing workers they could keep a secret, and some were senior staff rather than line workers, which made them read as management.
The economics of the factory floor worked against the Champions. Productivity in these factories is measured by team, so a Champion who steps away from the line costs every person on their team money. Champions did their health work at lunch and on breaks, squeezed between quotas. Almost all of them told us they wanted training, as long as it happened on non-work days.
Assumptions were blocking care. HR staff, and some Champions, believed unmarried workers didn't need family planning information, on the assumption they weren't sexually active.
Paper died in drawers. Every infirmary had the program's counseling flipchart out and in constant use; staff loved it. Nearly every other paper resource was out of sight. The program had also distributed Android phones with a referral app, and staff had forgotten the passwords or quietly gone back to paper referral slips.
 The counseling flipchart, the one paper tool every infirmary actually used.
The counseling flipchart, the one paper tool every infirmary actually used.
 The method-choice spread: options ordered by effectiveness, icons doing the work instead of text.
The method-choice spread: options ordered by effectiveness, icons doing the work instead of text.
And the group chat. The peer support infrastructure already existed, built by the users themselves, on the platform they already opened every day.
What we built
For the clinic and infirmary staff: a mobile-first e-learning platform, built on WordPress because open source keeps it maintainable after the consultants leave. Marie Stopes' training content became modules with courses, certification and discussion groups, and their team got admin tools to add content themselves. It was designed for the phones the program had already put in staff hands, with user guides in Khmer and English.
For the Champions: a training program that costs half a day per year, on a Sunday, because we knew exactly what an hour off the line costs. It taught trust-building habits alongside the health content. The program's existing "We Are Brave, We Are Smart, We Can Do It!" brochure became a set of revision cards that Champions practice explaining to each other as a game. Each Champion also got a One-Sheet guide: a single Khmer-language page with communication tips, key family planning facts and a fill-in map of the referral contacts in their own factory.
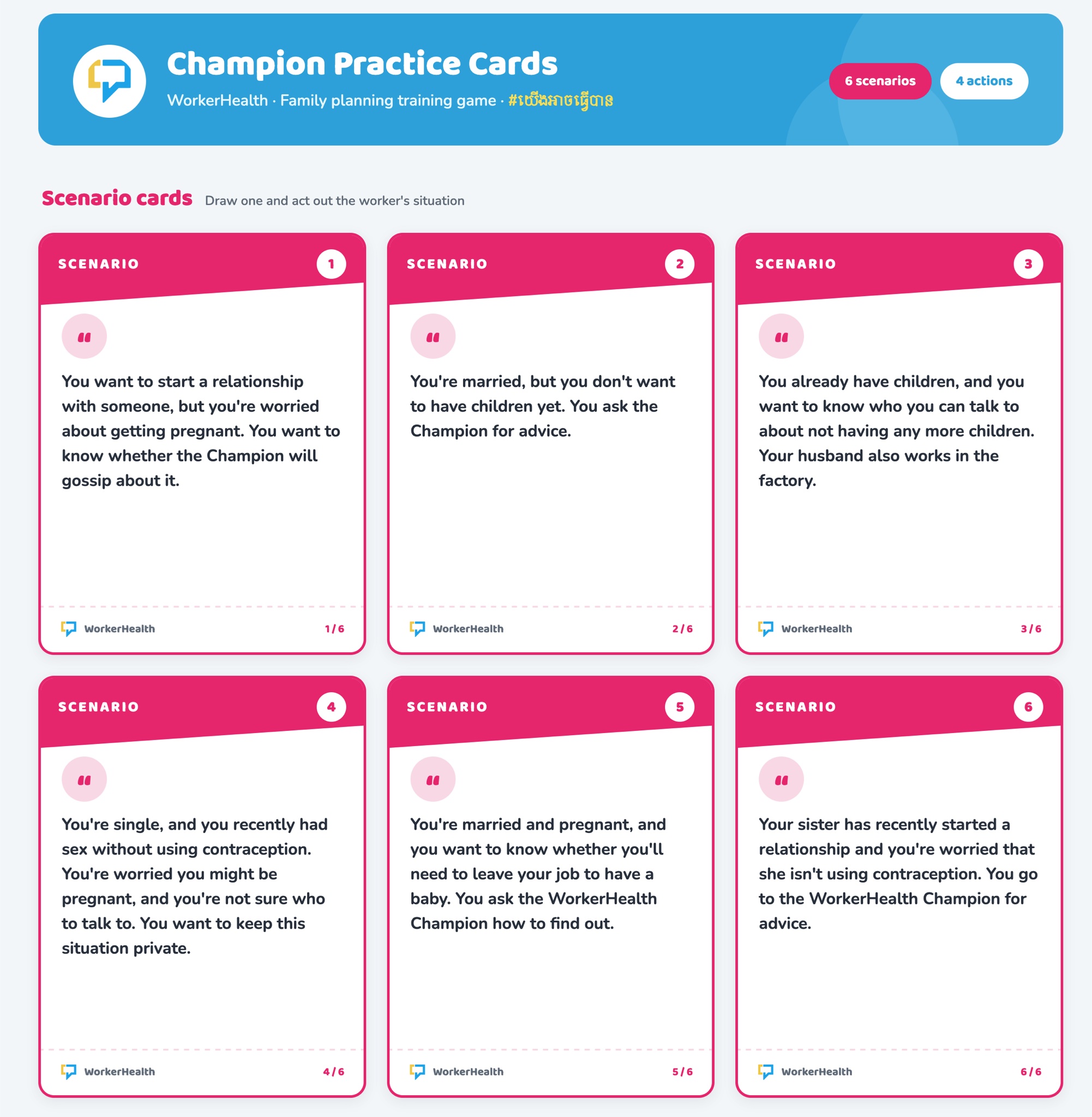 The practice game's scenario cards: one Champion draws a worker's situation and acts it out.
The practice game's scenario cards: one Champion draws a worker's situation and acts it out.
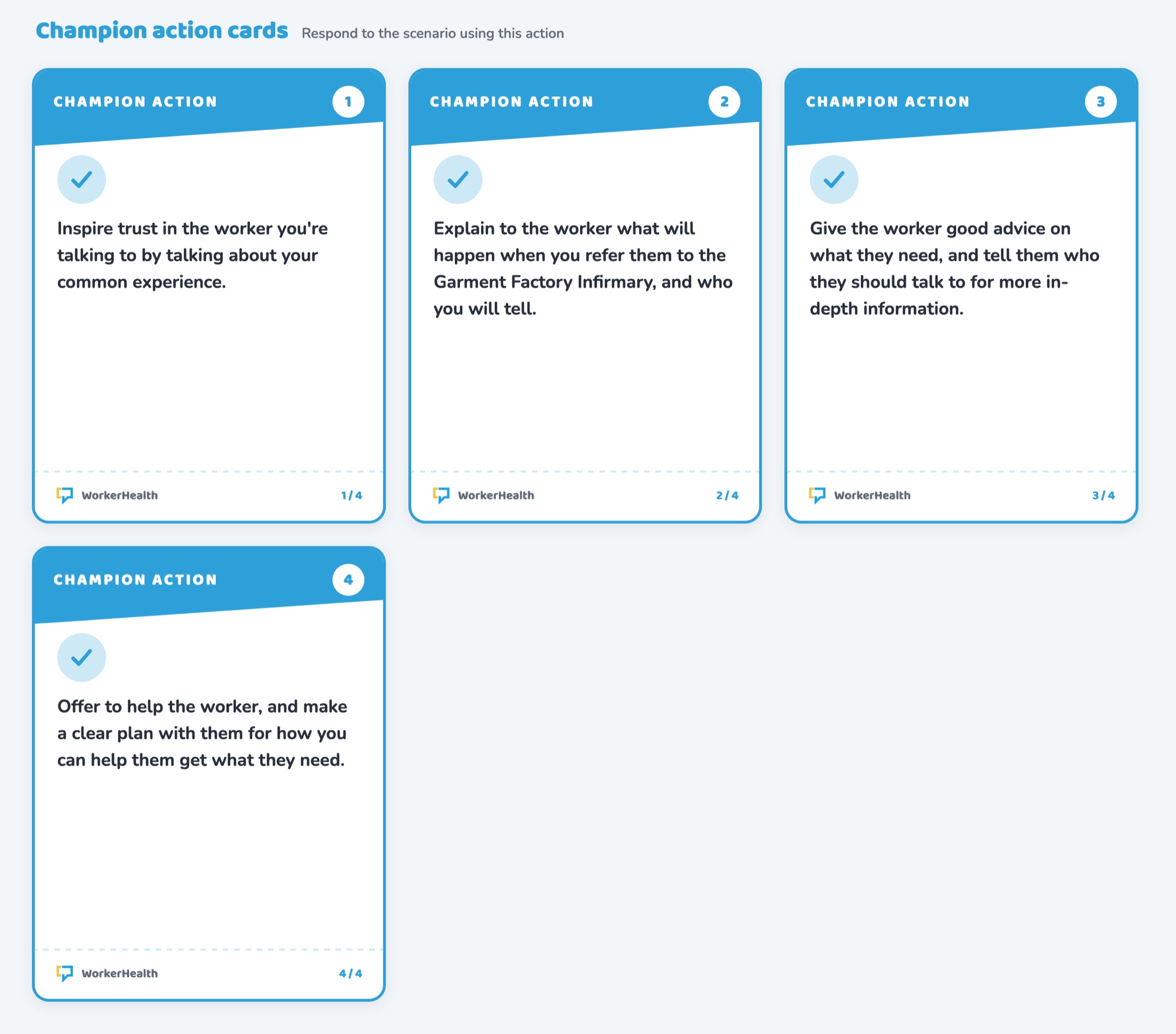 The action cards: the other Champion responds using one of four trust-building moves.
The action cards: the other Champion responds using one of four trust-building moves.
For factory management, we mostly didn't build. Strong tools already existed (a government-endorsed toolkit, infirmary guidelines, a business case) and were sitting unread. We designed a guide, a poster and a network mapping tool whose whole job was to make those existing tools visible and give HR staff the language to pitch health programming upward: healthy workers, better factories.
We closed with training-of-trainers sessions for each tool in early 2018, then spent three days on-site at the Marie Stopes office while their team took over the platform.
What it taught me
The timeline had one pass of research and one pass of design in it. No returning to test the tools in the factories before handover. Our final report recommended ongoing iteration, and I still think about what a second round of testing would have caught.
Design where people are, not where you'd like them to be. The most valuable piece of infrastructure in a multi-year, donor-funded health program was a group chat a few factory workers set up themselves, for free, because they needed it. We didn't build it. Our job was to notice it, respect it, and build everything else around it.
Working on something like this?
Research, design or a good question. All welcome.